In the knee there are 4 main groups of ligaments that are responsible, in conjunction with the knee cartilages and muscle control, for stability of the knee joint.
 First published 2010, and reviewed in October 2023 by Dr Sheila Strover (Clinical Editor)
First published 2010, and reviewed in October 2023 by Dr Sheila Strover (Clinical Editor)
The ACL and PCL sit in the middle of the knee and are surrounded by joint fluid (synovial fluid). When the ligament snaps/ruptures/tears the ends retract back, leaving a gap in the middle. This gap cannot be bridged by repair tissue because the gap is too big and is also full of joint fluid. For this reason ACL tears rarely ever heal.
If a knee ligament is torn, then the result is frequently that the knee feels wobbly and unstable, and gives way recurrently. Each time the knee gives way there is the risk that more damage is being caused to the structures inside the joint, in addition to the risk of sustaining additional injury to other bones and joints from falling over.
Although some individuals can compensate for ligament injury if their muscles are strong enough and their reflexes quick enough, many will have ongoing instability that will have a significant effect on sporting participation or their daily activities.
Ligament reconstructions
Ligament reconstructions in and around the knee have been performed by surgeons for many years. During this time the techniques for ligament reconstruction have evolved significantly. Reconstructions can now be performed often as a day case or with just a single night's stay in hospital. In most cases good or excellent results are expected with high levels of return to sports participation after appropriate rehabilitation.
The majority of ligament reconstructions currently undertaken in the United Kingdom are performed by using tendon 'grafts' harvested from areas around the injured or opposite knee.
It is important for patients to recognise however that a number of different graft options are available.
Different graft options
There have been lots of scientific studies looking at whether hamstring tendons are better than patellar tendon grafts, or vice versa. The overall analysis confirms that good outcomes can be obtained with both choices. Patellar tendon grafts have the advantage that they may heal and become more firmly fixed a little quicker than hamstring grafts and their size and shape may be a little more predictable. The downside of having a patellar tendon graft is that taking the graft requires an incision (scar) at the front of the knee. Some patients can suffer ongoing pain at the front of the knee and discomfort kneeling after an ACL reconstruction if a patellar tendon graft has been used.
When a hamstring graft is used, a relatively thin strip of tendon is taken from the back of the knee/thigh. Two tendons are usually taken; the gracilis and the semitendinosis. These two are sewed together and then the strips are folded in half, giving 4 strands of tendon, which provides enough strength to replace the missing ACL. Newer modern devices for fixing the tendon in place give extremely strong fixation. The loss of the hamstring tendons from the back of the knee causes some loss of hamstring strength initially after the operation. However, the rest of the hamstrings very rapidly compensate during the post-operative rehabilitation period so that soon no actual weakness can be noticed.
Donors are screened very carefully indeed to exclude individuals from any high risk category for carrying any kind of infection. Blood samples are taken to check for the presence of bacterial or viral infections. The tissue is taken by an aseptic technique, meaning that it is removed from the donor in a sterile fashion (in the same way that surgery is performed in an operating theatre).
The tissue graft itself is then tested for a very wide variety of diseases, bacteria and viruses. Any positive results mean that the tissue will be discarded.
Tissue that has cleared this process is then subjected to a sterilisation process. The grafts are then frozen and stored in an accredited Tissue Bank. The freezing process helps sterilise the tissue even further.
The National Blood Service has estimated that the risk of any graft potentially being contaminated and carrying any kind of infection is as low as approximately 1 in 1 million. Various tendons are available as allografts, giving the surgeon a very wide choice of types, sizes, lengths and strengths.
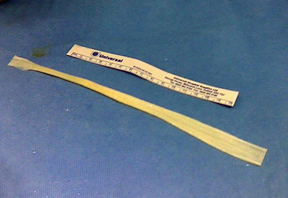
These photographs show a Tibialis Anterior Tendon Allograft before and after preparation.

What are the benefits of using allografts?
When a surgeon uses an allograft for an ACL reconstruction, it means that they do not have to harvest tendon tissue from the actual patient. This means that :
- Scars can be much smaller.
- The operating time is significantly shorter.
- Patients do not have to suffer the additional pain from the site of where the tendon was taken from.
- Reconstructions can be performed where multiple grafts are required.
- They can be used where the patient's tendons have already been used or have been damaged.
This means that patients undergoing ligament reconstruction with an allograft tend to have less post-operative pain, be more mobile sooner, and make a quicker recovery with faster rehabilitation.
A number of clinical outcomes studies have now been published that show that the healing and functional results of using allograft tendon tissue are just as good as using autograft tendon tissue taken from a patient's own body.
What are the potential downsides of using allografts?
There is some evidence that allograft tendon tissue may potentially weaken a little faster or a little more than autograft tendon in the first few months directly after the ligament reconstruction operation. However, within a further few months the allograft tissue gets remodelled and becomes strong again, in just the same way as autograft tissue does. Furthermore, allograft tendons actually tend to be significantly stronger than the average autograft:-
| The ultimate tensile strength (Newtons) | |
| Normal ACL | 1500 – 2000 |
| 4-strand Hamstring Allograft | 2000 – 3000 |
| Tibialis Anterior Allograft (my preference) | 2000 – 4000 |
Therefore, there is actually more leeway for allografts to weaken during the remodelling phase of recovery anyway. In practice, the concept of degradation and remodelling very much tends not to be a relevant practical issue.
One potential issue with the use of allograft tissue such as donor kidneys or other such organs is the need for tissue matching and immunosuppression. This is where great care has to be taken to match the tissue type of the donor tissue to the recipient patient's tissue type, in order to avoid rejection. In addition, very strong immunosuppressive drugs have to be given to the patient, to dampen down their immune system.
Fortunately, with allograft tendon tissue the processing techniques for sterilising the grafts and the freezing process for storing them kills all of the cells in the tissue. Furthermore, the cells and the material from the cells (such as proteins) are locked in a dense bed of material (matrix) within the tendon tissue. Therefore, with allograft tendon tissue there is no need for tissue typing or for immunosuppressive drugs, and the graft simply acts as a relatively inert scaffold in the knee into which the patient's own blood vessels and cells grow. If one were to take a tissue biopsy from an allograft tendon a few months after surgical implantation, the DNA typing would be entirely the same as the patient's own profile, i.e. the tissue has become part of the patient's own tissue.
Infection is always a concern in all fields of surgery, and when using donor tissue there is a potential concern about the risk of diseases or infections being passed on in contaminated grafts. All allograft tissue is subject to the stringent rules and regulations of the E.U. Human Tissue Act. The UK National Blood Service has estimated that the potential risk of receiving blood from a donor where the blood is actually carrying an infection (after having gone through its stringent processes) is approximately 1 in 3 million. Whilst similar specific data is not readily available for tendon allografts, RTI Biologics, one of the major allograft suppliers, has stated that there has been a zero incidence of allograft-associated infection in more than a million implants used. Also, to-date there have been no reported cases of transmission of diseases due to prions, such as Creutzfeld-Jakob Disease (CJD / Mad Cow Disease).
The main potential practical downside of using allograft tendons is their cost, with each graft costing somewhere in the region of £2000+. However, a study by Cole et al (Arthroscopy 2005) analysed the overall healthcare economics of the use of allografts for ACL reconstruction. They noted that the use of allografts led to shorter operating theatre times and a reduced average length of hospital stay, and concluded that the use of allografts was less expensive overall than using autograft. The most direct and apparent cost from the patient’s perspective, however, is the initial cost of the graft, which is charged by the hospital to the patient or their insurance company. This is, therefore, an issue that does have to be bourn in mind and duly considered by each individual patient.
In my practices in London and in Northwood, the approach that I take is to explain the various issues above to my patients, combined with directing them to further information on our website – www.sportsortho.co.uk
Patients are then actively encouraged to e-mail me back with any remaining questions that they might still have. I leave it entirely up to each patient to choose and to tell me what graft type they might like me to use for their reconstruction. In the revision setting or for complex multi-ligament reconstructions, allograft is by far the most common choice for grafts. In the primary setting, approximately 50% of my patients are now choosing allograft tendons for their ACL reconstructions.
Patients are then actively encouraged to e-mail me back with any remaining questions that they might still have. I leave it entirely up to each patient to choose and to tell me what graft type they might like me to use for their reconstruction. In the revision setting or for complex multi-ligament reconstructions, allograft is by far the most common choice for grafts. In the primary setting, approximately 50% of my patients are now choosing allograft tendons for their ACL reconstructions.
In Summary
Knee ligament injuries are a common problem. When undergoing ligament reconstruction surgery, there are a whole host of various options that must be discussed with your surgeon in detail before going ahead. One important discussion is about what type of graft is going to be used.
This information is intended solely as a general guide, to inform you about the general relevant issues. However, the actual choice as to what type of graft to use for any individual surgical ligament reconstruction procedure is a very important decision that must be discussed in detail between the patient and their surgeon, as each surgeon, each knee and each patient are always different.
Further reading:
Poehling et al. ‘Analysis of Outcomes of Anterior Cruciate Ligament Repair with 5-year Follow-up: Allograft versus Autograft.’ Arthroscopy 2005; 21(7): 774-785 This study showed that the long-term results of using autografts and allografts are very similar. However, those patients receiving allografts had less pain in the early post-operative period (6 weeks), better function at 1 week, 3 months and 1 year, and fewer activity limitations throughout the whole follow-up period.
Cole et al. ‘Cost comparison of anterior cruciate ligament reconstruction: autograft versus allograft.’ Arthroscopy 2005; 21(7): 786-790 This analysis found: “Allograft reconstruction of the ACL was significantly less expensive than autograft bone-patellar tendon-bone reconstruction. Allograft ACL reconstruction is a less costly alternative to autograft reconstruction.”
Dr (Mr) Ian McDermott

Mr Ian McDermott is a Consultant Orthopaedic Surgeon specialising purely in just knees. Ian left the NHS in 2007,...read more