This article covers key concerns about arthrofibrosis of the knee.
 Article written in 2019 by Dr Sheila Strover (Clinical Editor) and reviewed in September 2023.
Article written in 2019 by Dr Sheila Strover (Clinical Editor) and reviewed in September 2023.
What is arthrofibrosis?
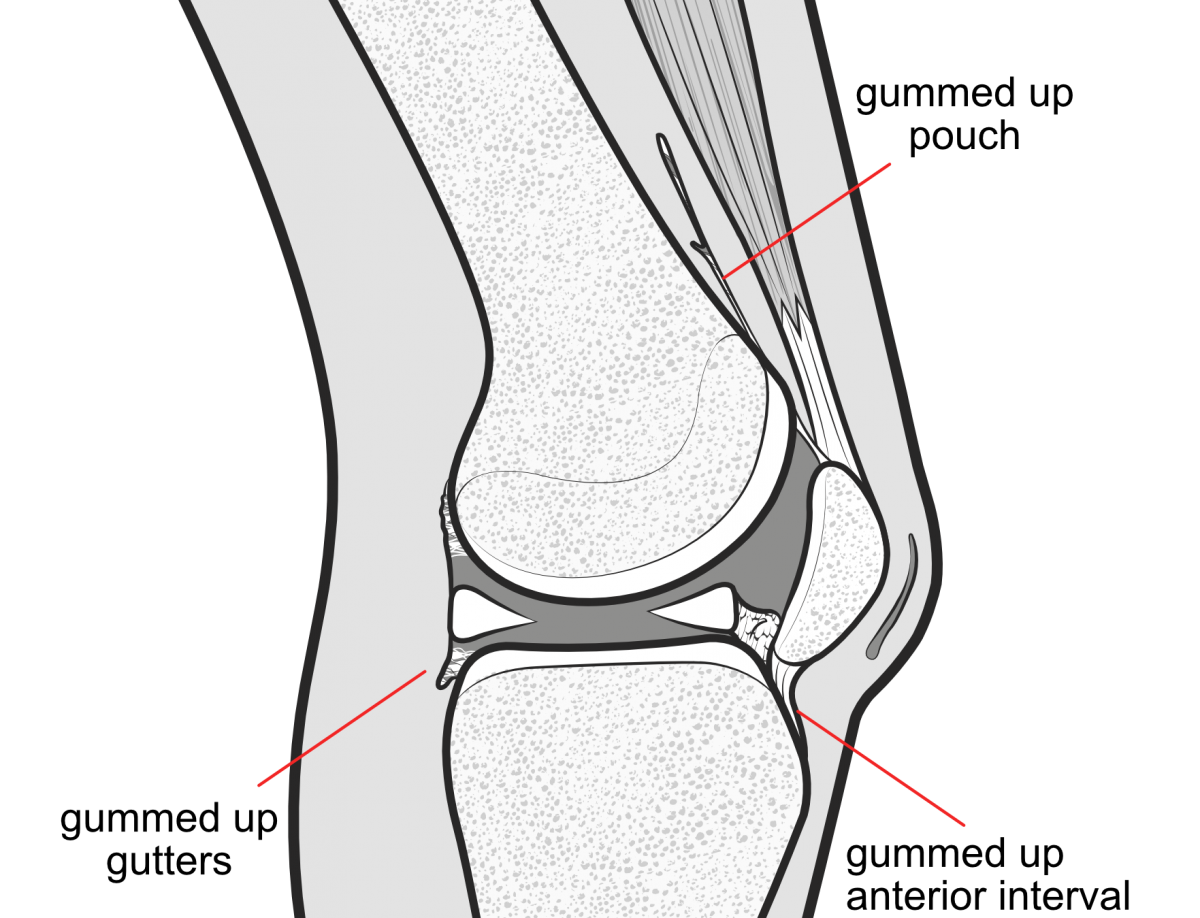
Arthrofibrosis (AF) is abnormal internal scarring inside the knee joint and surrounding structures. It may begin with sticky adhesions that can gum up the surfaces that are close to one another, such as the suprapatellar pouch above the patella, the anterior interval behind the patellar tendon, the area around the cruciate ligaments and the capsular 'gutters' at the side of the joint.
The abnormal 'gumminess' of these normally mobile tissues leads to painful knee stiffness. Attempts to bend the knee result in sickening pain above the knee in the region of the suprapatellar pouch. Aggressive physiotherapy tends to make the knee hot, swollen, red and painful, and instead of mobility improving it tends to worsen. Lack of understanding about the arthrofibrotic process may lead to doctor and physiotherapist berating the patient for not trying hard enough, and the patient may feel demoralised and angry.
Doctors commonly describe the extent of arthrofibrotic involvement using grading systems such as that developed by by Dr Donald Shelbourne and a complementary one by Dr Norman Sprague.
What triggers knee arthrofibrosis?
There seems to be two kinds of AF. One is a 'primary' type, probably with a genetic origin, where the person involved may have noticed that they tend to scar skin wounds very readily but then go on to 'over-scar' to form ugly kheloid scars - when this type of person has adhesions triggered in the knee their progress is more aggressive than the 'secondary' type of AF. The secondary type seems to have definite physical triggers that involve a traumatic incident, such as injury or surgery, prolonged use of a tourniquet during surgery, an abnormally long period of immobilisation of the knee, infection and finally inflammation which is aggravated during rehabilitation attempts to re-mobilise the joint. Certain procedures definitely carry an increased risk.
How common is knee arthrofibrosis?
You will find online reports that this condition is rare - but this is false. The genetic type of arthrofibrosis that is highly aggressive and confounds the physiotherapist and surgeon probably is quite rare, but the less aggressive type is more common and physiotherapists are becoming more aware of it, and ready to refer the patient back to the surgeon before it is too late.
After anterior cruciate ligament injury, AF has been reported with an incidence from 4% to 35%, and it is a predominant reason for re-operation for a stiff knee after total knee replacement.
Arthrofibrosis of the knee following ligament surgery. DeHaven KE, Cosgarea AJ and Sebastianelli WJ. Instr Course Lect. 2003;52:369-81.
Range of motion problems after ACL reconstruction
Range of motion problems after anterior cruciate ligament (ACL) reconstruction may be the result of poor surgical technique, placing the graft in a functionally poor position or using a graft that is an inappropriate width. Roughly 2% of ACL reconstruction patients have stiffness sufficient to require surgical intervention such as manipulation under anaesthesia or lysis of adhesions. Female patients carry a higher risk. Prevention involves decisions about when to do the surgery, focusing less on the length of time between ACL injury and surgical reconstruction and more on how inflamed the knee is at the time of surgery - it is important for the knee to be 'calm' when doing the initial reconstruction. Rehabilitation focuses on regaining range of motion without flaring up the knee. The physiotherapist will mobilise the tissues around the kneecap via patellar mobilisations, and will being very sensitive to the need both the gently mobilise the knee but all the time avoiding triggering a backlash from inflammation. The physiotherapist will also refer the patient back to the surgeon when there is a problem with limitation of extension.
Procedural Intervention for Arthrofibrosis after ACL reconstruction: Trends over Two Decades. Sanders TL, Kremers HM, Bryan AJ, Kremers WK, Stuart MJ, MD and Krych AJ. Knee Surg Sports Traumatol Arthrosc. 2017 Feb; 25(2): 532–537.
Use of Knee Extension Device During Rehabilitation of a Patient with Type 3 Arthrofibrosis after ACL Reconstruction Biggs A and Shelbourne KD. N Am J Sports Phys Ther. 2006 Aug; 1(3): 124–131.
Arthrofibrosis after total knee replacement
A stiff knee from arthrofibrosis after a total knee replacement can be devastating to the patient who has anticipated recovery of function after years of arthritis. Besides loss of range of motion, there may be considerable pain because of tethering of the normally mobile walls of the suprapatellar pouch, the lateral gutters and the anterior interval (behind the patellar tendon). Manipulation under anaesthesia (MUA) can be dangerous as it may cause fracture of the femur or rupture of the patellar tendon, so it has to be used with care only in the early stages if physiotherapy is not effective in mobilising the knee. Arthroscopic lysis of adhesions may free enough to allow physiotherapy to advance, but it may become necessary to open the knee to remove the scar tissue or even revise the knee replacement.
Stiffness after total knee arthroplasty. Bong MR and Di Cesare PE. J Am Acad Orthop Surg. 2004 May-Jun;12(3):164-71.
Arthroscopic Arthrolysis for Arthrofibrosis of the Knee after Total Knee Replacement. Hegazy AM and Elsoufy MA. HSS J. 2011 Jul; 7(2): 130–133.
Physiotherapy for knee arthrofibrosis
When symptoms of heat, pain and stiffness worsen despite physiotherapy, it becomes time for the astute physiotherapist to notify the referring doctor, so that close monitoring of the situation can be instituted. Efforts should focus upon adequate pain relief and breaking down adhesions without inflaming the knee - in particular patellar mobilisations should be skilfully performed and taught to the patient, so that the suprapatellar pouch and the soft tissues in area around the patellar tendon are kept mobile. Stretches at this stage to improve range of motion are more important than worrying about muscle strength or endurance. Every attempt must be to calm down the angry knee - anti-inflammatory medications, icing before and after rehabilitation sessions, shorter but more frequent sessions.
Perioperative Rehabilitation Using a Knee Extension Device and Arthroscopic Debridement in the Treatment of Arthrofibrosis. Biggs-Kinzer A, Murphy B, Shelbourne KD and Urch. Sports Health. 2010 Sep; 2(5): 417–423.
Capsular insufflation
This is the procedure of inflating the joint space within the capsule with fluid under pressure, in order to stretch and break any early adhesions.
Manipulation under anaesthesia
The objective of manipulation of the knee (MUA) is to break sticky adhesions gumming surfaces together before these adhesions turn into proper scar tissue. To this end the procedure should be done early once it is appreciated that physiotherapy is no longer improving range of motion (ROM) or that ROM is getting worse. During the procedure the patient needs to be fully anaesthetised and under the influence of true muscle relaxants. The hip should be bent to 90 degress and the surgeon hold the thigh near the knee and apply a gentle rocking motion of the lower limb through flexion and extension while observing improvement.
Here is a video showing an MUA of a sedated patient performed by Dr Ty Talcott. Not every practitioner will perform the manipulation in exactly the same way. By having the patient under anaesthetic or deep sedation, the clinician is able to gently but firmly take the knee through as much of a range of motion as possible in order to free any adhesions. A danger of course is that the inexperienced practitioner may be rough and cause damage to the tissues.
Manipulation Under Anaesthesia for Stiffness Following Knee Arthroplasty. Mohammed R, Syed S and Ahmed N. Ann R Coll Surg Engl. 2009 Apr; 91(3): 220–223.
Lysis of adhesions
In the early stages if manipulation fails, the surgeon may undertake a debridement to free the adhesions.
Although the simple procedure is not often considered, capsular insufflation or distension - filling the knee under pressure with saline to stretch and pop adhesions - is something that might also be tried in the very early cases before a manipulation, debridement or LOA is considered or in the operating theatre just before continuing with surgery.
Lysis of adhesions (LOA) (melting or breaking down the adhesions) in the knee can be performed both arthroscopically (keyhole surgery) or via open surgery. The procedure involves using a burr, punch or laser 'wand' to break the adhesions in the suprapatellar pouch above the kneecap, intercondylar notch around the attachment of the cruciate ligaments and lateral gutters to the side of the joint. This allows these soft tissue areas to mobilise the the patient should regain initial range of motion, which then needs to be maintained with a regime of pain management, and physiotherapy.
Arthroscopic Lysis of Adhesions for Treatment of Post-traumatic Arthrofibrosis of the Knee Joint. Stiefel EC and McIntyre L. Arthrosc Tech. 2017 Aug; 6(4): e939–e944.
Arthroscopic Arthrolysis for Arthrofibrosis of the Knee after Total Knee Replacement. Hegazy AM and Elsoufy MA. HSS J. 2011 Jul; 7(2): 130–133.
Arthroscopic Lysis of Adhesions for the Stiff Total Knee Arthroplasty. Enad JG. Arthrosc Tech. 2014 Oct; 3(5): e611–e614.
Prognostic Factors of Arthroscopic Adhesiolysis for Arthrofibrosis of the Knee. Kim Y-M and Joo YB. Knee Surg Relat Res. 2013 Dec; 25(4): 202–206.
Hydraulic distension of the knee: a novel treatment for arthrofibrosis after total knee replacement (case series). Formby PM, Donohue MA, Cannova CJ and Caulfield JP. ANZ J Surg. 2016 Jun;86(6):480-2. doi: 10.1111/ans.13540. Epub 2016 Apr 12.
The role of capsular distention in the arthroscopic management of arthrofibrosis of the knee: A technical consideration. Millett PJ and Steadman JR. Arthroscopy. 2001 Sep;17(7):E31.
Anterior interval release

Anterior interval release is a surgical procedure to release scar tissue in the anterior interval behind the patellar tendon, in the normally-mobile area bordered by the femur behind and the tendon in front. The area is accessed by the surgeon through a keyhole portal, and the curtain of scar tissue just in front of the intermeniscal ligament is melted away until the tissues are freed and range of motion improved.
Surgical Technique for Release of Anterior Interval Scarring of the Knee After Anterior Cruciate Ligament Reconstruction. Rose M, McNeilan R, Genuario J and Schlegel T. Arthroscopy Techniques September 2018 Volume 7, Issue 9, Pages e887–e891. NB there is a nice video available to download as an mp4.
Posterior capsulotomy
When there is scarring in the posterior gutters, the patient may be unable to fully extend the knee (extension deficit) unless adhesions are released in the capsular gutter at the back of the knee. The procedure is generally performed via an open incision where the adhesions can be visualised and palpated, and then surgically released. A further manipulation may be necessary to ensure that full extension is achievable, and rehabilitation is focused upon retaining full extension.
Posterior Capsulotomy of the Knee: Treatment of Minimal Knee Extension Deficit. Gomes JLE, Leie MA, de Freitas Soares A, Ferrari MB and Sánchez G. Arthrosc Tech. 2017 Oct; 6(5): e1535–e1539.

Relevant dictionary entries -
- Arthrofibrosis
- Manipulation under anaesthesia (MUA)
- Lysis of adhesions (LOA)
- Anterior interval release (AIR)
- Capsulotomy

Video - What is arthrofibrosis?
A 15-minute overview in simple language, with audio - by Dr Sheila Strover (Clinical Editor).
eBook - How to perform Patellar Mobilisations
Free downloadable eBook by Mr Sebastiano Nutarelli (Physiotherapist), fully illustrated with explanations of the mobilisation exercises.

Video-based course on Udemy - The stiff knee after injury or surgery
If video is your preferred learning medium, this detailed course may suit you. Presented by Mr Sebastiano Nutarelli (Physiotherapist) and Dr Sheila Strover (Clinical Editor).

List - Who's Who in arthrofibrosis surgery
Contact details of knee surgeons known to have a particular interest in the management of arthrofibrosis of the knee.