This is a course on knee realignment osteotomy, but osteotomy can also play a role in realigning the patella in its groove.
 First published 2010, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published 2010, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Realignment osteotomy for knee pain - course
Part 1 - Introduction to the subject of knee osteotomy
Part 2 - Osteotomy for varus and valgus deformity
- Indications for varus and valgus osteotomy
- Living with painful varus and valgus deformity
- High tibial osteotomy and distal femoral osteotomy
- Case study of high tibial osteotomy aiding ligament instability
- Benefits of varus/valgus osteotomy
- Potential problems with varus/valgus osteotomy
- Recovery post knee osteotomy
Part 3 - Osteotomy for patellar instability
- Patellar instability and dislocation
- Dislocators with normal anatomy prior to dislocation
- Dislocators with abnormal anatomy prior to dislocation
I am focusing this discussion primarily on patients who are patellar dislocators, although I touch on procedures that also relate to people who have patellar instability and are subluxators but who do not necessarily experience full-blown dislocation.
Normal anatomy before dislocation
If you have a completely normal knee and you fall over and injure it and your patella becomes unstable as a result, that’s a relatively straightforward issue to resolve. The damage is likely to be to the inner patellar support structures, the most important of which is the medial patello-femoral ligament. There is a fairly new ligament procedure that treat such traumatic instability with, and that is medial patellofemoral ligament (MPFL) reconstruction. MPFL reconstruction is the 'new ACL' of knee surgery and lots of different techniques have been designed. We are now on 'technique mark 4' and it seems to work well. I will discuss this in the next section of this part of the course.
Abnormal anatomy prior to dislocation
Then there is this other group of people that have patellar instability and who basically have abnormal anatomy – they have a flat trochlea ( V-shaped groove on the femur where the patella runs), or their patellar tendon is too and their tibial tubercle is too lateral. The anatomical abnormalities can be described as -
Proximal (on the femur)
The trochlea is flat and there is no groove for the patella to run within. This is a pretty rare condition and is termed trochlear dysplasia. The procedure we use to treat this condition is a trochleoplasty. In this procedure the trochlear ‘V’ shaped groove is surgically re-created so that the patella and its tendon can sit in it and remain stable throughout the range of knee motion. Trochleoplasty is a niche operation - most of us carry out tubercle osteotomies but there are only three surgeons in the UK that frequently carry out modern trochleoplasty - Pete Thompson is one ( Coventry and Warwickshire Hospital), Jonathan Eldridge in Bristol is the other and Simon Donnell in Norfolk and Norwich is the third.
 Distal (on the tibia)
Distal (on the tibia)
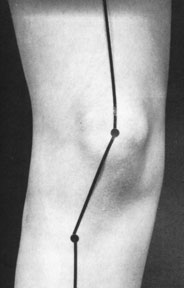
In these people the patella tendon is positioned too far laterally (to the outer side). This is picked up clinically by the 'q angle' (quadriceps angle). The q-angle is calculated by drawing a line from the pelvis (exactly from the anterior superior iliac spine - that hard bit you can feel on the front of pelvis) and the middle of the patella and then a second line down the middle of the patella tendon to the tibial tubercle where the tendon inserts. The upper 'normal' figure for the q-angle is approximately 15 degrees.
Much more important than the q-angle is the tibial tubercle transfer distance. This is the distance from the middle of the tibial tubercle to the middle of the trochlea and is calculated by CT scan. The magic figure is 20mm. Less than this and you can get away with an MPFL reconstruction. More than this and you need a distal realignment osteotomy such as a modified Fulkerson procedure. Most surgeons would also do a lateral release +/- medial tightening or reefing.
Most patients with abnormal patello-femoral anatomy have valgus alignment and are knock kneed. The patella is not central and is instead tilted laterally, and there is a degree of rotational malalignment. The key to stabilising the patella is to to deal with the trochlea if it is dysplastic/flat or with the tibial tubercle if it is laterally placed.
A patient may say "Shouldn't they deal with my knock knees to stop the dislocations?" - and the answer is that this is very rarely necessary. At the experts masterclass in osteotomy, that I attended in Zurich last year, one surgeon described a case where the patella dislocation was missed and the patient presented with a patella that had been dislocated for 2 months. The surgeon did a var-ising distal femoral osteotomy on the femur to correct the knock knee and then was able to do to a modified Fulkerson and an MPFL to get the patella in the groove - where it stayed.
I will go into these two groups of patient in a bit more detail as we move forward in the course.
The importance of Imaging
When assessing a knee we always get four different X-ray views. One of them, the skyline view of the patello-femoral joint (a special X-ray where you look down on the knee) does not give you as much information as we once thought. We all now tend to rely on the lateral knee X-ray more than anything else. Then we send the patients for an MRI scan and try and find answers to the following questions : “Is the trochlea dysplastic?”, that is “Is it too flat, or is it humped?” or “Is it truly ‘V’shaped as it should be?”. We also look at the quality of the cartilage, and we look critically at the tibial tubercle transfer distance (TTTD). The magic figure for this is 20mm. If a patient's TTTD is less than 20 mm then they will tend to do well either with conservative management or if that fails, with a soft tissue MPFL reconstruction. If that figure is greater than 20mm and the patients has failed conservative management then those patients do tend to do well with surgery. Surgery for someone who is skeletally mature is some form of bone realignment procedure, very occasionally adding in an MPFL reconstruction, but usually the bony procedure is enough. What will determine which bony procedure depends really on where most of the deformity is.
The French surgeon, Henri Dejour, was the one who worked out that this lateral X-ray is the key to evaluation. He came up with this sign called the ‘crossing sign’ (or Dejour’s sign). His son, David Dejour, is now one of the top knee surgeons in Lyon and France.
Professor Adrian Wilson

KNEEguru CONTRIBUTOR
Mr Adrian Wilson is a consultant knee surgeon based in London in the UK. His practice involves...read more