Published 2004
A young soccer player finds himself frustrated, unable to find out what is wrong with his knee.
After submitting to extensive physiotherapy and two lots of surgery he finds out that his symptoms are due to a thickened plica.

J.L. is a 16 year old schoolboy. He is a talented sportsman, playing soccer, tennis, squash and running to keep fit.
About 18 months ago he tried to get fit enough to compete in middle distance athletics but had to give it up because he developed pain in his right knee which developed after running. The pain was quite severe and was situated above the knee cap and on the inner side of the knee. The pain was aggravated by going downstairs but not by going up. He was unaware of any swelling, but said that the knee felt hot on occasion. The pain was associated with a regular click under the kneecap. He noticed the clicking more in the morning on first getting up and going downstairs to the bathroom. Besides the pain and clicking, J.L. noticed that his knee became stiff and ached when he sat in one position for any length of time.
Struggling for a diagnosis
J.L. sought treatment from the club physiotherapist (PT) who taped the kneecap and gave him V.M.O exercises (vastus medialis obliquus - ie the inner quads muscle). Although this seemed to help in the first instance, as time went on the exercises made the pain worse and his physio suggested that he sought advice from a podiatrist as J.L. had pronated (flat) feet which is known to often aggravate knee pain. The physio felt that the problem might be corrected by appropriate inserts into his footware.
J.L. spent £300 (about $500) on inserts for his shoes and trainers but his knee pain got worse until he noticed that he could only run about a mile or play soccer for about 20 minutes before the pain stopped him from continuing the exercise. Pain on stairs was becoming an everyday occurrence and J.L. stopped playing soccer and stopped jogging.
He sought advice from his G.P. (primary care practitioner) who did some blood tests and prescribed anti-inflammatory tablets, rest and ice. The pain and clicking settled down during this period, but immediately returned when he went back to sporting activities. He asked for a referral to an orthopaedic surgeon with an interest in sports medicine.
Surgery fails to reveal diagnosis
This orthopaedic surgeon examined J.L.'s knee and suspected chondromalacia and maltracking of the patella, or else some damage to his joint surface or his meniscal cartilages. He ordered an X-ray, which was normal, and an M.R.I. scan which was also reported as normal. He decided to do an arthroscopy as a day case.
The arthroscopy showed normal appearances to the meniscal cartilages, ligaments and joint surfaces, but the surgeon took photographs and kept a video of the procedure. He also did a biopsy of the synovial membrane.
The biopsy showed 'non-specific synovitis' (inflammation without obvious cause) and the surgeon advised that a steroid injection into the joint might help.
The injection into the knee did help for about 6 weeks, but then the symptoms came back.
More rehab but still no diagnosis
The surgeon sent J.L. to another physiotherapist, who decided to do an isokinetic test. This tests the muscles working the joint at maximum strength at a pre-determined speed through a full range of movements. The test was painful and the physio asked J.L. to score the pain on a scale of 1 to 10. J.L. said that at its worst the pain was about 5 out of 10.
Again he was given quadriceps exercises, but J.L.'s pain returned when he went back to playing squash and running.
J.L. was persuaded to have another arthroscopy during which this surgeon inspected the joint from an entry portal (small surgical cut) above the kneecap. A thickened plica was found and a video showed the entrapment of the plica between the patella and the femur whilst the knee was being bent to 90 degrees.
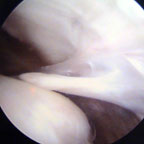
Plica showing contact with the bone
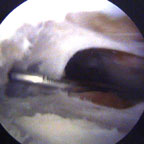
Plica from below - it often has a 'window' like this
