Looking at the many ways that a knee surgeon is exposed to training.
 First published in 2013, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published in 2013, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Skills training in knee surgery
How does a knee surgeon gain mastery over a new surgical procedure when it takes time to familiarise oneself with complex instrumentation and techniques?
It is not acceptable to practice on patients, but it is equally not feasible to take the expensive equipment away from the operating room for practice sessions. How also to shortcut the process of understanding the issues and controversies and the potential surgical pitfalls?
Hands-on skills workshops provide an answer. An experienced team of surgeons will put the event together, and if it is successful and gains a good reputation they will continue to improve it and run it annually or even more frequently. Delegates may travel long distances to attend a popular workshop, and either pay the fee themselves or gain funding from their employer. Any shortfall is topped up by the support of key industry players in that particular field.
The host team often invite a hand-picked faculty of experts, drawn from all over the world. These enthusiastic pedagogues generally give their time without remuneration, although their travel and accommodation expenses would be funded from course revenues. The workshops follow a fairly standard format, may run over a number of days and include -
Plenary sessions
The plenary sessions allow delegates to settle into the topic, and to get to know what to expect from the course.
Introduction of the host faculty
The local hosts will introduce themselves and outline how they developed their own particular interest in the subject. Invariably, they will respectfully mention their own past mentors and usually come up with some humorous anecdotes about them. This serves to emphasise the importance of 'fraternity' amongst members of such a speciality.
Fig1. - Knee surgeon, Adrian Wilson, senior convenor of the annual Basingstoke osteotomy workshop.
The guest faculty, often international, will then be introduced, with some coverage of their own institutions and particular interests. It is taken for granted that they are open to visits from colleagues with a special interest in their work, and they may mention their own fellowship programmes, usually 6-12 months of specialist training in their organisation.
The theoretical element
Each member of the faculty will make a presentation (usually of the Powerpoint variety but well illustrated, including photos, X-rays and videos), together covering the background history, relevant anatomy, key issues and controversies, key pitfalls, key books to read, key papers in the literature, key experts in the field, further anecdotes about relevant heroes, and differences in practice between countries.
Fig2. - Knee surgeon, Neil Thomas, also a very knowledgeable medical historian, talking about the history of osteotomy.
Question and Answer sessions
These would be facilitated by one of the faculty or perhaps another mentor. Microphones would be available to members of audience, who introduce themselves before posing their question.

Case Presentations
After the usual coffee breaks, members of the faculty are likely to present some of their own clinical cases. This introduces a true life dimension, and involves the delegates in decision making, based on their understanding of the issues so far explained. There might be videos of patients, images of the pre-surgical planning, videos of the actual surgery and the post-operative follow up. Occasionally a real patient will be prepared to come onto the podium and be involved.
These sessions are usually lively and bring out many points of discussion. A good facilitator will know which experts in the audience should be handed the microphone to bring out all the issues and controversies.
Practical demonstrations
If there is a special technique or detail of instrumentation that will be of interest to the delegates, a demonstration work-table might be set up. The surgeon will explain the details, while a larger video is relayed to the main screen. The equipment will have been provided by one of the trade organisations supporting the meeting.

Fig 3. - Knee surgeons Konrad Synarski (Poland) and Robert Litchfield (Canada)
Here two guest faculty members demonstrate a surgical technique in which they have particular expertise. In this instance, the delegates have been split into two teams and there is plenty of intimacy to come up close and ask questions of the experts.
Decision-making practicals
As part of any skills meeting, there may be an element where the surgeons have to decide how they themselves might approach a surgical problem.
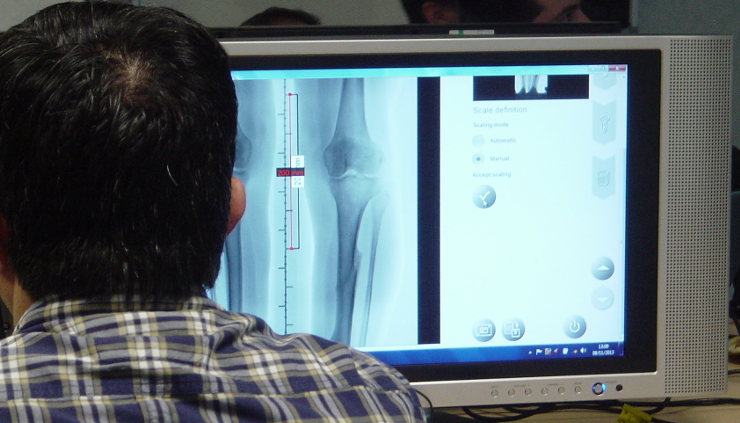
Fig 4. - Learning to use the surgical planning software for a knee osteotomy
Here delegates learn to use a computer system to work out on real X-ray images how they would plan their osteotomy cuts.
Hands-on skills workshops
This is the key element of the course from the perspective of the delegates. As this example is an osteotomy course involving the cutting and re-positioning of bones, a 'dry-bone' session is appropriate, with the bones being commercial foam products and not real bones. Some courses involving soft tissues will instead use cadaver knees, so that the surgical experience is authentic.

Fig 5. - Delegates practising in teams.
The key trade sponsor will have supplied the meeting with a full set of instrumentation for each pair of delegates, who will assist one another in following the steps explained by the demonstrator. The tutor's workstation will be projected onto large screens, so that everyone can follow the procedures, while facilitators move from pair to pair to help to guide the surgery to a good conclusion. Such facilitators may include operating room staff and members of the relevant trade team.

Fig 6. - Ronald van Heerwaarden from the Netherlands demonstrating an important point.
A really important element of meeting like these is that the individual surgeons get to meet global experts in the field, interacting with them on a truly personal level. A point is much more likely to be remembered when it comes from a very respected colleague.
Demonstrations at trade tables
The industry sponsors of such a meeting are true participants, because they have helped to develop the products and instrumentation, they have travelled the world attending such meetings and have followed the presentations many times, and they are intimately known to the operating room staff who of course order products from them and rent the surgical instruments.
Relayed live surgery
If appropriate, and especially at larger meetings near key hospitals, there will be a relay of a live surgical procedure, with video and two way microphones, so that delegates can follow the procedure and ask questions as the surgery progresses.
By events such as these, a very strong bond of friendship and fraternity develops between all these participants. At meetings elsewhere in the world the delegate will be able to approach these mentors with confidence and build on their own knowledge base. They will visit one another, and invite one another to join their own faculties as they develop in their field.
PREVIOUS PART: Who's Who in posterolateral corner surgery
END OF PRIMER.
