Continuing instability after cruciate ligament reconstruction may be the result of a missed complex lateral tear. The KNEEguru editorial team offers an interpretation of this medical paper by a group of Spanish doctors who use a neat model to explain the mechanics of these complex instabilities.
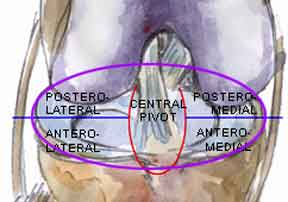
To understand the clinical scenario when several of these are simultaneously disrupted in an injury it is useful to consider the knee in terms of quadrants around a central pivot area.
Imagine that you are looking down at the top of the tibia from above and you have divided the tibial plateau into four quadrants around a central pivot area.
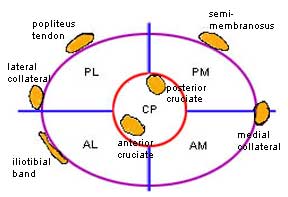
If you look at it schematically, with several of the restraints positioned, it is easy to see what quadrant is unstable if a restraint is damaged -
AL - anterolateral AM - anteromedial Pl - posterolateral PM - posteromedial CP - central pivot
Although medial instabilities occur more frequently than lateral instabilities, they are more readily diagnosed and easier to treat. The difficult complex instabilities are those of the lateral quadrants -
- A tear of the capsule, ilio-tibial band and the anterior cruciate ligament results in anterolateral instability
- A tear or avulsion of the capsule, lateral collateral ligament, popliteus tendon and a cruciate results in posterolateral instability. Also contributing to postero-lateral instability, but not marked on the diagram are detachments of the superior rim of the tibia ('Segond fracture') and tears of the biceps femoris.
The mechanism of injury in anterolateral instability is frequently a fall forward, with the foot on the ground twisted inward and the knee joint prised apart on the outer side towards the front.
The mechanism of injury in posterolateral instability is either -
- A direct blow (eg kick) on the inner aspect of the knee while the foot on the ground is twisted outward, prising the knee apart at the outer side towards the back OR
- The straight led being suddenly forced backwards (hyper-extension) while the foot on the ground is twisted inward.

Often missed...
