Dr Noyes highlights the fibular collateral ligament and the popliteus muscle-tendon-ligament unit as key structures of the posterolateral corner.
 First published 2009 by Dr Frank R Noyes, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published 2009 by Dr Frank R Noyes, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Posterolateral corner injuries of the knee - course
- What the posterolateral corner is and why it matters
- Key structures of the posterolateral corner
- Biceps femoris in relation to posterolateral corner structures
- Relationship of biceps femoris to the structures of the posterolateral corner
- The structures of the posterolateral corner
- Mechanism of injury of the posterolateral corner
- Managing posterolateral corner injuries without surgery
- Surgery for posterolateral corner injuries
- Outcomes after posterolateral corner injury
Related course: Rehabilitation protocol after posterolateral corner surgery
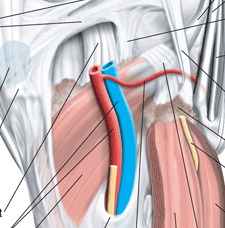
There are many structures that make up the posterolateral region of the knee joint.
The most important in terms of knee stability and function are the fibular collateral ligament and the popliteus muscle-tendon-ligament unit.
Studies from our laboratory and others have shown that these two components are responsible for limiting (or restraining) abnormal lateral joint opening and external tibial rotation that I discussed in Part 1. When these abnormal knee motions occur, patients suffer from the knee collapsing, pain, difficulty with walking, and other serious problems. Therefore, it is important that when surgery is required, these structures are reconstructed with high strength grafts to restore stability. In some cases, the fibular collateral ligament may be ruptured, but the other structures are intact or just somewhat loose. These knees only require a single graft to replace the ligament. I will talk more about surgical options in Part 5 of this course.

Fibular collateral ligament (FCL)
The FCL (also termed the lateral collateral ligament, or LCL) is a cord-like ligament that runs from the lateral femur to the fibular head (see Figure).
This ligament prevents the femur and tibia from coming apart at the lateral (outside) aspect of the knee joint and it also prevents the tibia from rotating outwards.
[This article was published in Noyes’ Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes, Noyes FR, Barber-Westin SD (eds.), Copyright Saunders, 2009 - Noyes FR, Barber-Westin SB: Posterolateral ligament injuries: Diagnosis, operative techniques, and clinical outcomes, pages 577-630.]
Fabellofibular ligament
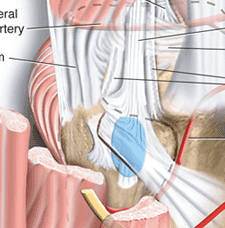
The fabellofibular ligament is one of the posterolateral corner structures, and I include it here although it is a small structure and there have been no biomechanical studies published that describe its function. The ligament begins at the lateral aspect of the fabella (a small bone like a mini-patella at the back of the knee) and it also inserts on the fibula.
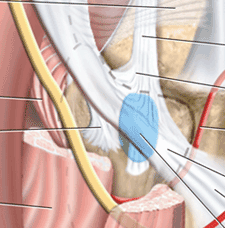
Popliteus muscle-tendon-ligament unit (PMTL)
The PMTL is made up of the popliteus muscle, the popliteofibular ligament (PFL), the femoral insertion of the popliteus tendon, the popliteomeniscal fascicles and soft tissue attachments to the lateral meniscus, and the proximal tibia.
Click here to see the full labelled illustration.
The popliteus tendon and PFL are the most important elements of this unit in terms of providing stability to the knee. These structures aid the FCL and posterolateral capsule to prevent excessive external tibial rotation and varus rotation. [That is, they keep the bones stable in that corner of the knee.]
When the PMTL is deficient, it must be reconstructed with a graft (in addition to a graft replacment of the FCL) to fully restore posterolateral corner function.
The popliteus muscle originates at the back of the tibia and proceeds around the side and up (lateral and proximal) to insert on the lateral femoral condyle. Its tendon proceeds on proximally through a gap in the coronary ligament of the lateral meniscus, then passes deep to the FCL to ultimately insert in front of and below (anterior and distal) to the insertion of the FCL.
The PFL originates at the musculotendinous junction of the popliteus and attaches to the medial aspect of the fibular head, where it lies deep to the fabellofibular ligament.
[This article was published in Noyes’ Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes, Noyes FR, Barber-Westin SD (eds.), Copyright Saunders, 2009 - Strickland JP, Fester EW, Noyes FR: Lateral, posterior, and cruciate knee anatomy, pages 20-43.]
Biceps femoris
on the left
The biceps femoris is a fusiform (spindle-shaped) muscle comprised of two heads: long and short. Both heads have complex attachments to the posterolateral aspect of the knee, as shown in the figures.
Click here to see the full labelled illustration.
The fibular head
The fibular head (very top of the fibula) is a key anatomic and structural component to the posterolateral knee for the surgeon. There are six important structures that attach to the fibular head: PFL, FCL, fabellofibular ligament, long head of the biceps direct and anterior arms, and the short head of the biceps direct arm.
Iliotibial band (ITB)
The ITB is a large fascial expansion that originates on the anterior superior iliac spine covering the tensor fascia lata muscle proximally and extending along the lateral aspect of the thigh. The ITB and lateral capsule are important structures that resist internal tibia rotation. In severe lateral knee ligament injuries, the ITB may become abnormally lengthened and require surgical restoration.
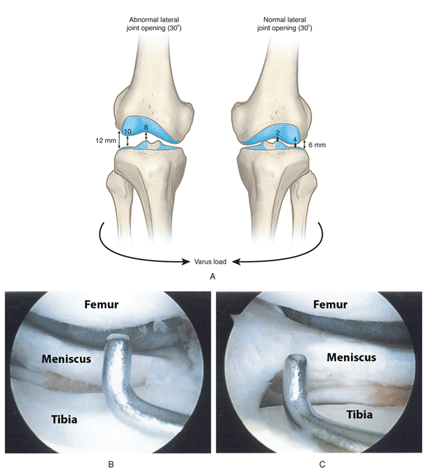
A diagram of abnormal lateral joint opening is shown here, along with an arthroscopic photograph of normal amount of joint opening (B) and abnormal joint opening (C). This is what I call the “gap test”, where during arthroscopy, I place a small amount of force on the knee to see how much the femur and tibia separate at the lateral part of the joint.
You can easily see the difference between the normal and abnormal joint opening in the photographs – the amount of space between the tip of the nerve hook and the femur. This is what happens when the patient is asleep and I place just a small amount of force on the knee. During actual activities such as walking, much greater forces are placed upon the joint and this is partially why these injuries an cause so much instability.
[This article was published in Noyes’ Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes, Noyes FR, Barber-Westin SD (eds.), Copyright Saunders, 2009 - Noyes FR, Barber-Westin SB: Posterolateral ligament injuries: Diagnosis, operative techniques, and clinical outcomes, pages 577-630.]

A patient with severe right knee hyperextension and external tibial rotation is shown in this example. The hyperextension the patient is able to produce during standing is shown in A, and the external tibial rotation is shown in B – see how far out the right foot rotates compared to the left? This is called the dial test and it is quite accurate for detecting posterolateral corner deficiency. I’ll talk more about the comprehensive examination required to detect PCL deficiency, as well as other potential problems in the knee joint a bit later.
PREVIOUS PART: What the posterolateral corner is and why it matters
NEXT PART: Biceps femoris in relation to posterolateral corner structures
Dr Frank R Noyes

DR NOYES HAS RETIRED.
Based at the Cincinnati Sportsmedicine and Orthopaedic Center in the USA, Dr Frank Noyes is one of the world's most prominent figures when it comes to knee surgery. A prolific researcher and writer, he has published over 200 studies and articles in the world's top...read more