When the suprapatellar pouch scars down, the patient will have a limitation of flexion. I want to make a few important points about this region -
- The scar tissue can be very dense and it can form underneath the muscles. The surgeon has to remove the scar tissue that is actually underneath the muscles of the quadriceps.
- In the suprapatellar pouch, a band may form which extends from the top of the patella (kneecap) to the top of the femoral condyles. It is a very dense band of scar tissue that has to be removed. This band or scar tissue may produce what we call a 'patellar clunk', where the kneecap clunks as it goes through flexion. The question is often asked if this represents actual damage to the joint. And the answer is - it may be damage to the joint, but it also may be just from the scar tissue located in that location. This same clunk may be present after total knee replacement, for the same reason.
- The knee joint also has a pouch on both the medial and lateral sides. I tell my patients these pouches are like your cheeks in your mouth - like the cheeks, they have a normal extensibility or flexibility and they are usually not really very tight.
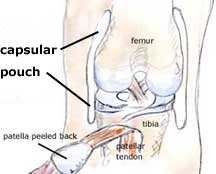
These pouches are anatomically called the 'capsular pouches' and during arthrofibrosis, they will scar down to the point of where they become adhesive to the side of the femur on both the medial and lateral aspects. Patients often complain that as they are trying to move their knee they feel tremendous stiffness - and they have - because their capsular pouches are adhesed down (adhered) to the side of the joint. The surgeon must open up those pouches to restore the normal gliding.
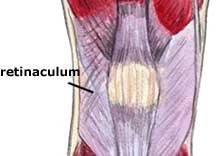
The patellar retinaculum is the fibrous tissue located on both sides of the patella -
Scar tissue in this region produces tremendous stiffness and blocks flexion. This scarring must be released nearly one-hundred percent of the time by the surgeon to restore a normal glide to the patellofemoral joint in a medial-lateral direction. It is very important if a patient does not have normal patellar glide, that they do not try to go past 100 degrees of flexion. This is because the tightness present in those tissues binds down the kneecap - forcing flexion may produce permanent damage to the joint.
One of the most important things that we do in our clinic is carefully stretch a knee joint, but with the recognition that in some patients, we will not be able to stretch out excessive scar tissue that is very firm and inelastic. To do so would be at the expense of the joint.
Remember, the goal of your treatment must be to preserve the joint lining (articular cartilage joint surfaces), because it is the joint lining itself that will completely deteriorate if you have a bound down knee. The medial and lateral patellar retinaculum must always be tested by the therapist and surgeon using the medial and lateral glide tests.
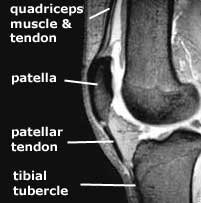
The next thing that produces a loss of flexion that is very difficult to deal with is shortening of the quadriceps muscle. We documented in our studies that the quadriceps mechanism and the muscle actually shorten because scar tissue prohibits normal muscle contractions and lengthening. This muscle may start to shorten as early as four months following an injury or operation. And before that, the patellar tendon also will begin shorten, resulting in what is termed a patella infera condition.
Once the quadriceps muscle/patellar tendon mechanism goes through this shortening process, it is extremely difficult to recover the normal length. Once the surgeon has released all the tissues that I just mentioned above, the final thing that may still be limiting flexion is shortening in the quadriceps muscle and patellar tendon.

It is very difficult to measure how much shortening has occurred in the quadriceps tendon. The surgeon can get an idea if he or she can only flex the knee ninety to a hundred degrees for example. However, one can measure the amount of patellar tendon shortening using a method we published many years ago. A lateral x-ray is obtained of both knees and the height of the patella is measured, which allows interpretation of the length of the patellar tendon. The measurement of the involved knee is compared with the opposite knee, and the resulting difference indicates the amount of patella infera present.
The second factor which may limit patellar tendon medial and lateral glide is adhesion of the patellar tendon to the tibia. The normal space is lost, requiring the surgeon to free up the patellar tendon. Otherwise, it will stick down to the tibia at the top of the joint rather than its normal postion at the tibial tubercle.





