Mechanism of injury of the ACL
A common mechanism of injury is sudden pivoting on that leg when the foot is on the ground and the weight on the same leg.
...a traumatic pivoting mechanism, typically without direct contact to the knee, a ‘popping’ or ‘snapping’ sensation, effusion within 2 h of injury and knee instability...".
How is a torn ACL diagnosed?
Firstly there will be a high index of suspicion - the patient may have had a high momentum injury, heard a loud 'pop!' and been unable to walk after the injury.
The knee may have immediately swelled up, and even after some days of rest the knee may feel unstable.
The clinician may test for laxity, classically using the 'anterior drawer' test. Laxity may also be tested objectively with an instrument such as the KT-2000
ACL tears are diagnosed by..."history and physical examination with imaging modalities utilised if required....the pivot shift and Lever sign tests demonstrate the highest diagnostic accuracy....anterior drawer, Lachman and Lever sign tests demonstrate similar diagnostic accuracy....other modalities (including MRI and arthrometry) are recommended when the history is suggestive of an ACL tear, but tests are negative".
Can a torn ACL heal on its own?
A partial tear of the ACL can heal on its own if the knee is protected from further damage.
Once fully avulsed or torn, the ACL is likely to require surgical repair or reconstruction.
"The effects of the timing of ACLR [ACL reconstruction] surgery on postoperative knee function and clinical outcomes continue to be heavily debated. Early ACLR may reduce postoperative complications in patients with ACL deficiency, whereas elective delayed reconstruction can decrease the risk of knee fibrosis and improve clinical results."
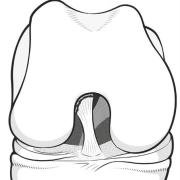
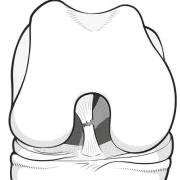
When is surgery indicated for a torn ACL?
Anterior cruciate ligament repair surgery is indicated in patients who have simply avulsed the ligament from the wall of the notch (Sherman Type I injury).
These patients are usually younger, and respond to a simple reattachment of the othewise undamaged ligament.
Ongoing instability in active patients with Sherman Type II-IV tears through the body of the ligament is likely to lead to reconstructive surgery with a graft harvested from the patellar tendon or hamstrings tendons.
The X-ray sign of a Segond fracture, indicating that the anterolateral ligament is also avulsed, will advise the surgeon of the need for the additional step of reconstruction of the anterolateral ligament, or else the isolated ACL reconstruction has a high chance of failure.
"....the main surgical indications described for ACL reconstruction combined with lateral extra-articular tenodesis or ALL reconstruction are: ACL revision, physical examination with pivot shift grade 2 or 3, sports practice with pivot movements and/or high-level sports practice, ligament laxity, and Segond fracture."
Forum discussions
- NO Pain and NO Inflammation: ACL/MCL Injury? - Several experienced ACL patients discuss how it is possible to tear the anterior cruciate ligament and not suffer severe swelling and pain during and after the incident.
- ACL and Meniscus surgery all at once -- or separate? - Different patient experiences about prioritising surgery for separate instabilities.