ACL injuries are usefully classified using the Sherman system.
The value of the classification system is that it helps to identify those patients who might benefit from an ACL repair rather than a reconstruction.
The Sherman classification is as follows:
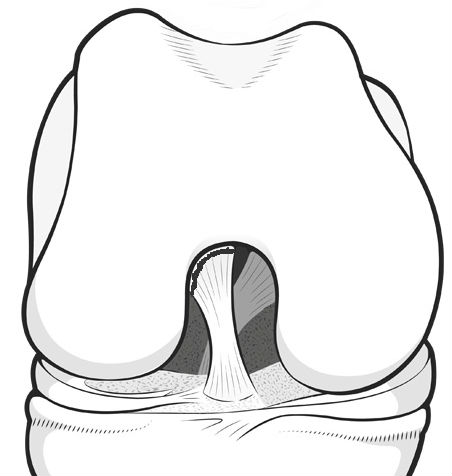 |
Type I is where the ligament literally pulls right off the bone from where it takes its origin in the notch of the femur |
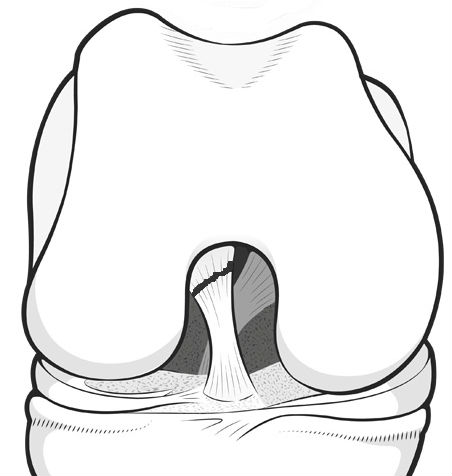 |
Type II is when the tear is close to, but not quite at, the attachment point on the wall of the femur. |
 |
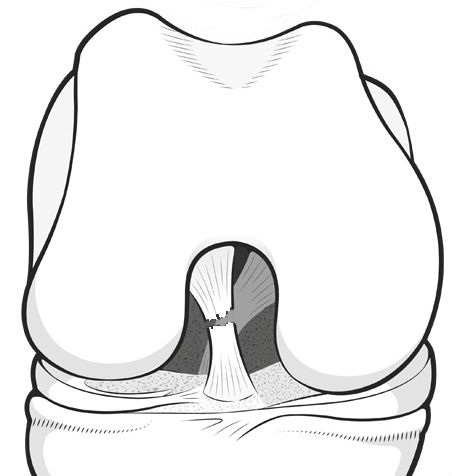
Type III is about a third of the way along the ligament |
 |
Type IV is a mid-substance tear, right in the middle of the ligament |
References
Sherman MF, Lieber L, Bonamo JR, Podesta L, Reiter I. The long-term followup of primary anterior cruciate ligament repair. Defining a rationale for augmentation. Am J Sports Med. 1991 May-Jun;19(3):243-55.
Sherman MF, Bonamo JR. Primary repair of the anterior cruciate ligament. Clin Sports Med 1988; 7:739–750

-