Mrs Lesley Hall explains what to expect at your first specialist appointment after injuring your cruciate ligament.
 First published in 2008, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published in 2008, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Cruciate Ligament Rehabilitation - course
Mrs Lesley Hall is a physiotherapist with a massive experience in knee rehabilitation.
- So you've torn your ACL?
- The early management of ACL tears
- Exercises in the early stage after ACL injury
-
Clinical assessment of ACL tears
- Torn ACL - should I have an operation?
- General principles of ACL rehabilitation
- Progressive rehab while deciding on surgery (I)
- Progressive rehab while deciding on surgery (II)
- Cruciate ligament rehabilitation - Rehab after surgery
Now that you have a bit more background, I am going to progress to the point of the first consultation, and discuss a little bit about the clinical assessment of the knee once the first fews days are over.
If you have given a good history your clinician will probably already have an idea what has happened before he examines you. He will always look at your opposite leg as well to make comparisons.
It has been suggested that approximately 35% of ACL injuries are missed on initial diagnosis!
Assessment of an acutely painful and swollen knee is not always easy - you can help your clinician greatly if you can give an accurate description of how the injury happened. He will not really be interested in where you were going when you slipped and fell but will be interested in the fact that your leg buckled and bent inwards, or that the bindings on your skis did not release as you fell backwards causing your knee to twist.
Reaching a diagnosis - the 'History'
The interesting points for the clinician are:
- the direction of any impact against the knee
- the direction the knee/leg moved
- the position you finished up in
- You will also be asked whether you heard any sound from the knee at the time of injury.
Knee noises are often described as:
Each of these descriptions may lead your doctor closer to determining which structure in the knee is damaged. Commonly, isolated ACL tears cause a loud 'popping' noise which is often heard by others in the vicinity.
Your surgeon will also want to know:
These are all important points which help to give an overall picture of the extent of injury.
Pain is obviously also important. The ACL is right in the centre of the joint and therefore pain is very difficult to localise. It is usually described as being deep and diffuse but the degree of pain felt at the time of injury is extremely variable from person to person. Some people describe sudden excruciating pain while others get up and carry on with whatever they were doing!! The ACL does have pain sensitive nerves but less pain does not necessarily mean less injury - sometimes a partial tear of the ligament is more painful than a complete tear, where the pain pathway is interrupted.
Finally your clinician will want to know about swelling. It may be that you are being examined very quickly after injury in which case any swelling will be obvious, but if there has been some time-lapse you may need to remember - did your knee swell and if so, over what sort of time frame?
Rapid swelling (within minutes) usually indicates some bleeding within the joint and is common in ACL injuries. Slower onset swelling (over hours) is due to excessive fluid production in the knee (inflammation) - this is your body's own attempt at healing. If your knee is swollen and tense at the time of assessment an aspiration may be carried out - this involves inserting a needle into the joint and withdrawing fluid. The benefits of this are twofold:
Examination

Palpating (feeling) the knee allows an assessment of swelling and inflammation - an inflamed knee may be very hot and tender as well as swollen.
The examiner will ask you to bend and straighten the knee as far as you can, he may then add some overpressure at the limits of your movement to check the full range. Any block to movement or pain will be noted as significant.
Typically your doctor or physiotherapist will test for cruciate ligament damage by assessing how far the tibia will glide forwards and backwards on the femur. Usually he will test both legs and compare them - this is because there is a natural difference in normal movement between different people, the examiner will use your uninjured leg to represent what is normal for you.
 |
Testing for the ACL is done with your knee bent approximately 20-30° from the horizontal. This test is called the -Lachman test' and is very sensitive and specific for the ACL. |
 |
Testing for the PCL (posterior cruciate ligament) is done with the knee bent at 90° and is called the 'Drawer test'. |
 |
There is another test which is very reliable for ACL injury called the 'lateral pivot shift' test. This involves applying a sideways pressure on the joint while rotating and bending it however, it can be difficult to perform in an acute situation or if a patient is very tense. It is more likely to be tried when examining a more chronic injury, or if assessing a joint under anaesthetic. |
Further diagnostic tests
Other investigations may prove necessary. Further diagnostic tests may be indicated to confirm a questionable diagnosis or to check if any other structures have also been injured - this could affect the treatment required.
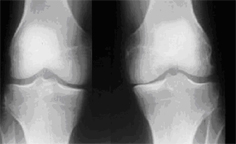
A Standard X-ray
This will only show bone but it may be important to rule out any fractures (breaks) and also to see how the bones are positioned in relation to each other. Sometimes a 'stress X-ray' is done to assess the integrity of the collateral ligaments - the X-ray is taken while sideways pressure is applied to the knee.
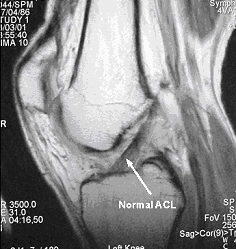
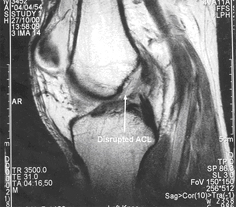
An MRI Scan
This will show all the structures in the knee and enables a reliable diagnosis to be made however, scans are very expensive and are not always available or if they are, there may be an unacceptably long wait.
A. The first image demonstrates an intact cruciate ligament.
B. The second image demonstrates a torn ACL.
Knee Ligament Arthrometry
The KT2000 is the most commonly used arthrometer to assess the ACL. The machine gives an objective measure of how much anterior tibial translation the ACL allows, again comparing with the uninjured side. The difference in movement between the two sides, with the same degree of force application, is the significant measure.
NB the examiner will always stand on the same side as the leg being tested - this photo was taken from the other side to allow visibility of the machine.
This is the end of Part 4 of this tutorial. In Part 5 I will walk you through the important process of making the decision about whether or not to have surgery.
PREVIOUS PART: Exercises in the early stage after ACL injury
NEXT PART: Torn ACL - should I have an operation?
Mrs Lesley Hall

Lesley Hall was a senior physiotherapist at the Droitwich Knee Clinic in Worcestershire, UK, but is now retired.
read more