Exercise bikes, static bikes, stationary cycles, bicycle ergometers - these are all names for the bicycles that you find in virtually every physiotherapy clinic, gym or health club across the world.
Many knee rehabilitation protocols include cycling so why is this exercise modality so popular for knee rehabilitation?
This article will give you an insight into the use of a cycle for knee rehabilitation. Firstly what we need to consider is that the broad goals of any knee rehabilitation programme are likely to be to -
- increase or restore knee joint range of movement
- increase or restore knee joint stability
- increase or restore the strength of muscles around the knee
- decrease or eliminate pain
- prevent reoccurrence of the injury
In comparison with other exercises cycling is a relatively 'knee friendly' activity that can help to improve knee joint mobility and stability. Cycling is frequently used as a rehabilitation exercise modality after knee injury or surgery as well as part of the management of chronic degenerative conditions such as osteoarthritis. The bicycle has a number of features that make it a particularly good tool for knee rehabilitation:
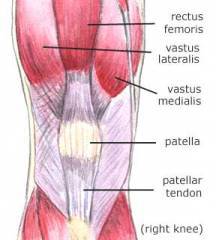
All of the major muscles of the legs are used at one point of another during cycling but the major muscles that are used for generating power are the quadriceps group, especially the quadriceps muscle rectus femoris (see diagram). During the pedal cycle the quadriceps mainly work as you push the pedal down and straighten your leg whilst the hamstrings at the back of thigh work to bend the knee. The amount the hamstrings work varies - if you are using pedals where your feet go under a strap your hamstrings work more as you can use them to pull the pedal up using the strap. By using cycling within the rehabilitation program the quadriceps can be strengthened whilst controlling the amount of stresses to the knee.
Knees like cyclical movement without excessive forces as that is the way that the articular cartilage covering the ends of your bones gets nourished.
Cycling has been shown to be a relatively safe activity for rehabilitation after anterior cruciate ligament (ACL) reconstruction as the strain that is placed on the ACL during cycling at rehabilitation levels is relatively low (Refs 4 & 5).
With the bike correctly set up during one complete turn of the pedal your knee travels from 30 to approximately 110 degrees of flexion. This can be seen in Figure 1. Before you can start to include stationary cycling in your knee rehabilitation you should have a minimum of 100 degrees of knee flexion so that you can complete one full turn of the pedals.
Saddle height
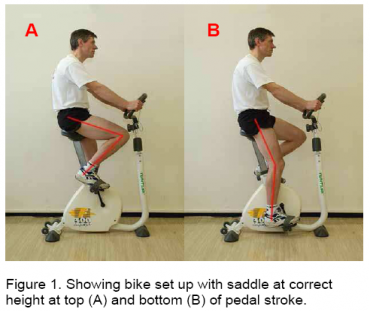 The height of the saddle on the bike has a direct influence on the amount of bend that occurs at the knee. If you take a look at the photos in Figures 1, 2 and 3 you can see the difference in knee angles when you alter the saddle height. Figure 1 shows the knee angles when the saddle is at the correct height. This needs to be set up for each person individually due to differences in leg length. We will show you how you how to set up the saddle height yourself a bit later on.
The height of the saddle on the bike has a direct influence on the amount of bend that occurs at the knee. If you take a look at the photos in Figures 1, 2 and 3 you can see the difference in knee angles when you alter the saddle height. Figure 1 shows the knee angles when the saddle is at the correct height. This needs to be set up for each person individually due to differences in leg length. We will show you how you how to set up the saddle height yourself a bit later on.
Saddle too high
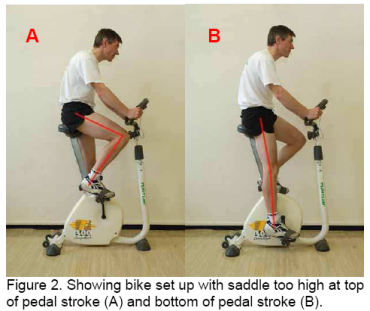
The main sign that your saddle is probably set too high is if when you are pedalling you find that your hips rock from side to side. This hip rocking can put extra stress on your hip joints. If the saddle is too high you will not be as stable on the bicycle which is not so much of a problem on a stationary bike in the gym but can be if you're cycling outside.
If the saddle is too high your knee will be almost straight when the pedal is at the bottom (Figure 2B) and the repetitive cycling action can irritate the iliotibial band (ITB) (Ref 1).
It has been shown that the strain on the ACL increases the more the knee straightens so having the saddle set too high puts even greater strain on the ACL (Ref 5).
Saddle too low
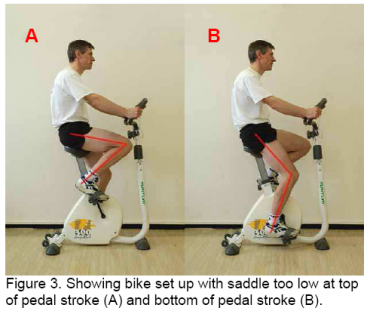
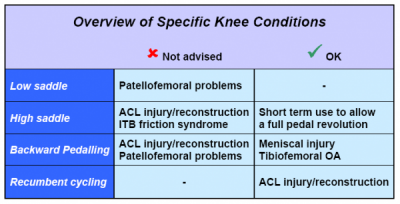
If the saddle is set too low the knee has to bend more. Compare the knee angle in Figure 3A compared to Figure 1A. This increased knee bend results in increased force going through the quadriceps muscle group and this results in increased stress on the patellofemoral joint (Ref 3). So anyone with patellofemoral problems should make sure that the saddle isn't too low as the cycling will aggravate the joint.
How to set up the saddle height
There are lots of magical formulas for working out the correct saddle height based on different variations of percentages of leg length. However, none of these calculations have been shown to work for everyone so the usual 'rule of thumb' for setting up saddle height is as follows:
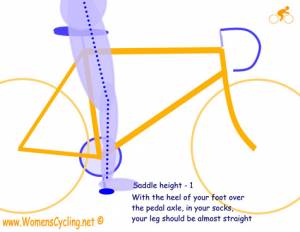
- Sit on the bike and allow one pedal to drop so that it is in the 6 o'clock position (as low as it will go).
- Place your heel on the pedal.
- In this position your knee should be almost straight but still have a slight bend (5-10 degrees). See diagram to right (courtesy of 'WomensCycling.net' which has since closed)
- Don't pedal with your heel on the pedal. This position is just used to set the saddle height.
- Now put your instep on the pedal and try a couple of turns. The saddle shouldn't be so high that your hips rock as you turn the pedals.
- Remember this is only a 'rule of thumb' guide so you may have to adjust things slightly dependent on your individual variation.
If you do have limited knee range of movement you may have to start off with the saddle slightly higher so that you are able to turn the pedal one whole revolution. If you do have to start off with your saddle a bit high what you should make sure is that as your range of motion of knee flexion increases you lower the saddle height until you are back at the correct height (Figure 1).
Backward pedalling on a stationary bike
Backward pedalling on a stationary bike is not a simple reversal of forward pedalling. Changing the direction of pedaling alters the relative contributions that the different muscles make to the activity.
When pedalling backwards, compared to forward pedalling, the quadriceps are even more active relative to the hamstrings (Refs 2 & 6). This increased quadriceps activity puts even greater stress on the patellofemoral joint so backward pedalling shouldn't be used for rehabilitation for anyone with patellofemoral joint problems. Also, when the leg is at its straightest point the ACL has less protection in backward pedalling compared to forward pedaling so backward pedalling is not recommended for anyone who has had an ACL injury or reconstruction (Ref 6). However, backward pedalling does reduce the pressure on the tibiofemoral joint so using backward pedalling on a stationary bike can be considered in the rehabilitation of meniscal problems or tibiofemoral osteoarthritis (Ref 6).
Recumbent cycling
A number of gyms and health clubs have recumbent cycles - these are the cycles where you sit in a chair with a backrest and the pedals are in front of you rather than below you as they would be in a standard upright cycling position.
There is no difference in the range of motion at the knee between recumbent and upright cycling. However, the change in position does alter the direction that forces are applied to the knee joint resulting in less load being placed on the ACL during recumbent cycling. It has therefore been suggested that recumbent cycling may be preferential to upright cycling in ACL rehabilitation (Ref 7).
The main points relating to the use of cycling for rehabilitation for different knee conditions are highlighted in the table below.
Getting back on the road
 There are a few things you should consider before progressing your rehabilitation from a stationary bike to a normal bike. When you can return to normal cycling is something that you can discuss with your doctor or therapist.
There are a few things you should consider before progressing your rehabilitation from a stationary bike to a normal bike. When you can return to normal cycling is something that you can discuss with your doctor or therapist.
Here are some general tips -
- For your own safety you need to be stable on the bike. Until you are stable stick to the stationary bike.
- Make sure your bicycle is set up correctly, especially the saddle height. If in doubt get a qualified bicycle mechanic to check your bike before you ride.
- Make sure that you are able to cycle for 30mins at a light resistance on a stationary bike without getting any knee problems before you switch to a normal bike.
- Hills put more stress on the knee joint so start off on a flat route.
- If your bike has gears you want to select a low gear that lets you turn the pedals around 90-100 times per minute (this is called the 'cadence'). If you pedal with a low cadence (less than 80 pedal revolutions per minute) more stress is put on the knee.
- Be sensible and build up the time and length of your cycle ride gradually.
- If the cycling does aggravate your knee remember the initial 'RICE' self treatment as soon as you get home.
If you have a permanent restriction in mobility in one knee or you have one leg shorter than the other there are special adaptations that can be made to the cranks and/or pedals.
References and Links
Ref 1. Asplund, C. & St Pierre, P. (2004) Knee Pain and Bicycling: Fitting Concepts for Clinicians. Physician and Sportsmedicine 32(4).View abstract.
Ref 2. Bressel, E. (2001) Influence of ergometer pedaling direction on peak patellofemoral joint forces. Clin Biomech 16(5):431-437. View abstract.
Ref 3. Ericson, M.O. & Nisell, R. (1987) Patellofemoral joint forces during ergometric cycling. Phys Ther 67(9):1365-1369. View abstract.
Ref 4. Ericson, M.O. & Nisell, R. (1986) Tibiofemoral joint forces during ergometer cycling. Am J Sports Med 14(4):285-290. View abstract.
Ref 5. Fleming, B.C. et al. (1998) The strain behaviour of the anterior cruciate ligament during bicycling. Am J Sports Med 26(1):109-118. View abstract.
Ref 6. Neptune, R.R. & Kautz, S.A. (2000) Knee joint loading in forward versus backward pedaling: Implications for rehabilitation strategies. Clin Biomech 15(7):528-535. View abstract.
Ref 7. Reiser, R.F., Broker, J.P. & Peterson, M.L. (2004) Knee loads in the standard and recumbent cycling positions. Biomed Sci Instrum 40:36-42. View abstract.
Specialist bicycle adaptations
Dr Karen Hambly

Dr Karen Hambly is a graduate sports scientist and HPC registered Chartered Physiotherapist with over 20...read more