There are many topics in the knee about which I am passionate, but I think this tops my list. Why? Well clinicians make a lot of mistakes here and patients suffer for it.
Kneecap pain seems a simple subject, but it is not. Correct diagnosis and treatment can make the difference between a cure and a wrecked knee.
Aimed at the level of patients, but also useful to clinicians, this course offers a comprehensive overview of the causes of pain around the knee cap, and what can be done to help patients suffering from knee cap pain. I have tried to strip it of 'med-speak' so that anyone can understand the topic, how it should be investigated and managed, where the pitfalls lie and how to avoid them.
The patella
Start now by examining your own knee cap -
Sit up on a bed where you can rest your back comfortably, with your legs out straight in front of you. With the leg straight, feel the boundaries of the knee cap. The knee cap can normally be wiggled from side to side in this position, and there is a good reason for this - in this high position it is above the groove of the trochlea, i.e. the groove in the underlying thigh bone along which the knee cap slides during its excursion when you are walking. [If you have dislocated your knee cap before, you will know to avoid doing wiggling it like this.] Bend your knee and now you will note that it is no longer possible to wiggle the knee cap. This is because the knee cap has now entered the groove of the trochlea.
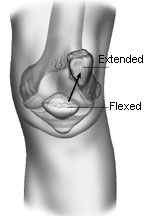
Here is an illustration of the knee area, showing the femur bone, with its rounded end and trochlear groove, and the position of the knee cap when the knee is straight (extended) and bent (flexed).
[Reprinted with permission from R. Grelsamer, MD, The Adult Knee, Ed. Callaghan JJ, Rosenberg AG, Rubash HE, Simonian PT, Wickiewicz TL, Lippincott Williams & Wilkins, Philadelphia, Chapters 59-60, Patellar Instability & Patellar Pain pp 929-949, 2003.]
See how in the straight position the knee cap does not really make contact with the groove, and in fact is way above the joint line. You can confirm that on your own knee. Then in the bent knee, the knee cap is guided into the groove.
On occasion, the groove is shallow or flat or even inverted. In other words, it is possible for the groove to be convex like a fried egg, in which case the knee cap can easily slip too far left or right (in which case the knee cap is said to be unstable).
Quadriceps muscle
Try squeezing your thigh. You can only feel the bone for a bit just above the knee joint. The rest is covered by muscles. The long bone of the thigh is the femur. The front of the femur is covered by four muscles that converge to the upper part of the knee cap, and, collectively, these are called the quadriceps (nickname: 'quads').
The 'quadriceps' muscle is the main muscle of the 'lap' and covers the whole of the front of the femur.
[The image on the left is reprinted with permission from R. Grelsamer, MD, The Adult Knee, Ed. Callaghan JJ, Rosenberg AG, Rubash HE, Simonian PT, Wickiewicz TL, Lippincott Williams & Wilkins, Philadelphia, Chapters 59-60, Patellar Instability & Patellar Pain pp 929-949, 2003.]
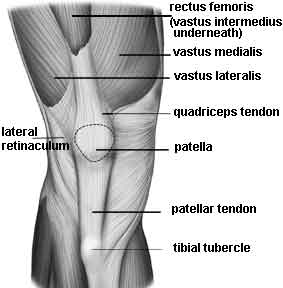
It is actually four muscles (quadri=4 ceps=heads):
- rectus femoris
- vastus medialis
- vastus lateralis
- vastus intermedius (not evident in the illustration)
They work together synergistically to straighten (extend) the knee.
Can you see the knee cap (patella)?
The patella is intimately related to the femur, and our simple illustration demonstrates the bones in relation to one another. The fibula is on the outer aspect of the lower leg, so on an X-ray it helps you identify whether you are looking at a right or a left leg.
 |
 |
The patella is connected above to the rectus femoris and to the vastus intermedius via a broad, flat tendon called the quadriceps tendon. At the bottom end, the knee cap is attached to the tibia (shin bone) by way of the patellar tendon, occasionally called the patellar ligament . This whole structure of the quads muscle with its embedded patella is known as the extensor mechanism, and it stretches from the bony attachment on the tibia just below the knee (the 'tibial tubercle') to the top of the femur near the hip. When the quadriceps muscle contracts this whole structure - the extensor mechanism - is tautened and the leg extends (straightens).
All the bundles of the quadriceps muscle tend to pull the patella up towards the head, but whereas the rectus femoris and vastus intermedius pull straight up, the vastus lateralis pulls the patella up and out, so to speak, and the vastus medialis pulls up and in. [Lateral means away from the midline, medial means towards the midline. Thus the little toe is lateral to the big toe, and the big toe is medial to the second toe.]
Lateral retinaculum and tibial tubercle
Take particular note of the lateral retinaculum and tibial tubercle in the illustration, because several of the surgical procedures we will discuss involve these structures. The tibial tubercle is also known as the tibial tuberosity.
Patellar Tendon
Just a word here on terminology ....
The peculiar anatomy of the patella means the structure below it is generally called a tendon, though it may also be called a ligament. Bands of tissue connecting one bone to another are called ligaments while bands of tissue connecting muscles to bone are called tendons.
Since the biological rope we are discussing connects the kneecap to the shinbone, in one sense, it is a ligament. On the other hand, functionally speaking, this rope is but a continuation of the quadriceps muscles (and of the quadriceps tendon). In this sense, our rope is a tendon, thus the term 'patellar tendon'.
PREVIOUS PART: Patellofemoral pain
NEXT PART: Important patellofemoral concepts
Dr Ronald Grelsamer

Dr Ronald P. Grelsamer, M.D., board certified by the American Board of Orthopaedic Surgery in 1987, is associate professor of orthopaedics at Mount Sinai ...read more
 Course first published 2008, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Course first published 2008, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Dr Ronald Grelsamer has decades of experience in managing problems of the knee related to the patella. In this course he gives a comprehensive overview of those conditions that can cause pain in the patellar region.