Repetitive cycling movement of the knee can lead to severe localised pain. Mr Willis-Owen explains...
 First published in 2012, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published in 2012, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Ilio-tibial Band Friction Syndrome is an overuse injury seen most commonly in runners and cyclists.
I have had firsthand experience of this when training for marathons and I have treated countless patients with the condition. I first experienced this when running on cambered road surfaces. I would get lateral knee pain a couple of miles into a run, and it would get progressively worse and cause me to have to stop. The pain was always well localised, and I experienced no click or snap.
I managed the situation by reducing my mileage by about 50% for a week and starting the Walt Reynolds regime. Each time it came on I would go back to the Walt Reynolds regime plus hip abduction exercises and eventually it completely settled.
Relevant Anatomy
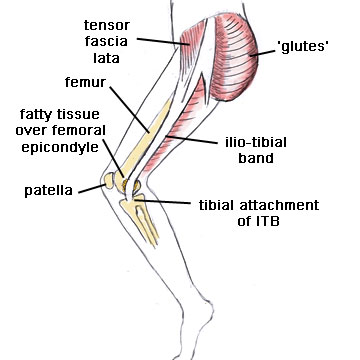
The iliotibial band (ITB) is a tight fibrous band of tissue running down the outside of the thigh from the pelvis to the tibia. It can cause friction as it crosses bony prominences - the two problem areas are the greater trochanter at the hip and the lateral femoral condyle on the outside of the knee. It is loading of the knee as the ITB cross the lateral epicondyle that causes increased friction.
Actually, relatively recent research points more to a compression against the lateral condyle of the femur than actual friction, but the theories are all a simplification and do not alter the management, and the name 'friction syndrome' has stuck.
Evaluation and management
Treatment involves first confirming the diagnosis, then establishing the cause. A skilled clinician can usually make the diagnosis from history and examination alone, only using an MRI scan to exclude any other problems. However all too often people get the MRI and rely on that to make the diagnosis, which either leads to treating an incidental finding or concluding that there is nothing wrong. It is quite easy to confirm the diagnosis if there is doubt by using a local anaesthetic injection to numb the ITB at the knee. If this solves your problem then you can be sure it is the ITB that is to blame.
Symptoms
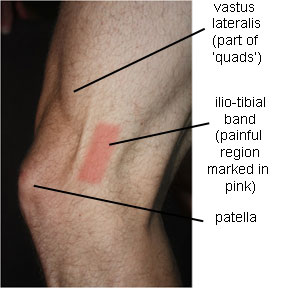
Patients feel pain on the outside of the knee, aggravated by activities that involve bending and straightening the knee repeatedly under load, such as running and cycling. Initially it may be a dull ache near the end of a session, but as the condition progresses the pain may be present more of the time and take longer to go away. They may notice it more running around corners or on camber, or cycling out of the saddle. There is a tender spot over the lateral epicondyle, but only with the knee flexed at 20-30 degrees (where the ITB lies over the epicondyle).
Aggravating factors
Tightness of the iliotibial band, biomechanical problems (over pronation of the feet, varus knees, or weak hip abductors), or certain training factors can bring this problem on.
Track running can be a culprit - always running in the same direction on the track puts more tension on the ITB of the outside leg and can be enough to bring the problem on. Similarly with road running, running on a cambered surface (such as the edge of the road) always with the same leg on the outside can trigger ITBFS. Downhill running (where the knee is at a lower knee flexion angle at heel strike) is often worse. Sprinting and speed work often feels better as heel strike occurs at higher flexion angles.
Cyclists can run in to trouble with imperfect cleat position putting more stress on the ITB. The problems can either be due to cleat rotation or the effective ‘Q’ factor – the distance between the balls of the feet being too narrow. Cleats with plenty of float may help.
Treatment
The first line treatment is relative rest and physiotherapy. As with all overuse injuries reducing training volume by half is a good starting point to allow the body to recover. Physio should concentrate on stretching the tight ITB, focus on quads and hamstrings control and address poor hip abductor control. There is a little known, but excellent exercise called the Walt Reynolds regimen, that I have found very helpful. This involves control aggravation of the ITB to try to stimulate a controlled healing response. The Walt Reynolds regime seems to be a well-kept secret in the UK, although it is well known in the USA.
Steroid injections to the area can help settle the inflammation down but should only be used in conjunction with physiotherapy and correction of the underlying problem.
Extra corporeal shockwave therapy is proving successful in a number of similar conditions. Again people are using it in the USA for ITBFS but it is not well used in the UK. It is not in widespread use for this at the moment, but I have a strong interest in this and expect it to prove to be a promising treatment.
In recalcitrant cases surgery is indicated. This can usually be performed as a minimally invasive daycase surgery. It involves removing a small triangle of the thickened posterior part of the ITB at the level of the epicondyle. Recovery is rapid with a graduated return to sport over 6 weeks.
Whilst you are recovering you must address the factors that caused the problem in the first place. Bike set up, running shoes, and running surfaces (road camber and track direction) and training regimen should all be scrutinised. ITB stretches, abductor strengthening and the Walt Reynolds regimen should become part of a regular routine to prevent recurrence
PREVIOUS PART: Patellar tendinitis
END OF COURSE.
Dr (Mr) Charles Willis-Owen

Mr Charles Willis-Owen is based in Poole and Bournemouth, UK. He is an orthopaedic surgeon but and also a keen triathlete, cyclist and an international elite marathon runner with considerable...read more