Patellar mobilisations are important in knee rehabilitation in order to prevent later stiffness of the joint.
 First published 2007, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
First published 2007, and reviewed August 2023 by Dr Sheila Strover (Clinical Editor)
Arthrofibrosis Rehab Tutorials
- Principles of arthrofibrosis rehabilitation
- Patellar Mobilisation
- Restoring Quad function
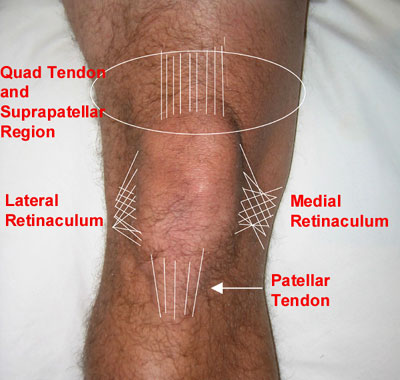
Adhesions that form under the patellar tendon, medial and lateral structures of the patella (or retinaculae), under the quad tendon and suprapatellar pouch, have been shown to decrease knee mobility and increase forces that occur between the patellar-femoral joint and tibio-femoral joint.
Increased forces between these joints can lead to accelerated wear on the joint cartilage.
Assessment and Mobilisation of the Patella, Quad and Patellar Tendons and Suprapatellar Region
Assessment of the patella should be done by shifting or gliding the patella in different directions. Our assessment includes:
- Medial glide - gliding the patellar toward the centerline of the body
- Lateral glide - gliding the patella away from the centerline of the body
- Superior glide - gliding the patella to the top of body
- Inferior glide - gliding the patella toward the feet
- Patellar Tendon - assessing the amount of movement of the patellar tendon medially and laterally
- Suprapatellar region - assessing the amount of movement of the region above the patella
General Guidelines for patellar mobilisations
Contraindications -
- If it is not recommended by your doctor or physical therapist
- Do not mobilize the patella laterally if you have had a lateral release procedure
- Do not mobilize the patella laterally if you have subluxed or dislocated your patella
- Avoid all mobilizations if you have had a quad or patellar tendon rupture or repair, unless this is cleared by your doctor or physical therapist
- Presence of a fracture
- Presence of an active infection
- Metastasizing malignancies
These are reasons NOT to mobilize (unless it has been cleared by your doctor or physical therapist)
Patella and tendon mobilizations are done to discourage adhesions from limiting motion (post-surgical) or to mobilize adhesions that have already formed to promote better mobility (post or non-surgical). When mobilizing your patella, or doing this for someone else, follow these guidelines:
- Try to mobilize to the maximal amount of excursion that the patella will permit without causing sharp or intense pain. A stretch or discomfort is allowed.
- Do not push down on the patella.
- Keep in mind that swelling will limit patellar mobility and knee motion - do not try to restore full patellar mobility if there is swelling present.
- Compare mobility to the uninvolved side to get an impression of what 'normal' mobility is (this is assuming that there is no underlying pathology on the 'normal' side). Decreased excursion in a specific direction is an indication to mobilize the patella or tendon in this direction.
- Mobilize in a comfortable, rhythmic motion. The speed of your mobilization is not important.
- Keep your quad muscles relaxed while mobilizing. Contracted quad muscles will 'lock down' the patella and place tension on the quad and patellar tendon making it difficult to mobilize these structures.
- Our protocol recommends doing the mobilizations for 5-15 minutes, 3-4 times per day. The mobilizations may cause discomfort from stretching tissue, but any intense or sharp pain should be avoided.
Medial Glide
When the lateral retinaculum is tight, you may feel that the patella tilts away from the center line. The opposite structures become mobilized when you move the patella laterally. These structures include the lateral retinaculum, lateral portion of the quad and patellar tendon tendons.
To mobilize the patella medially, place your fingers on the lateral border of the patella. This can be found by feeling for the edges of the patella with your fingers. Bring your fingers to the edge of the bone until they can not go any further to lateral edge. Now push the patella medially. Assess the amount of excursion of the patella.
Medial glide and tilt
When the lateral retinaculum is tight, you may feel that the patella tilts toward you. Decreased mobility or tilting of the patella is an indication to mobilize in this direction. A combination of a medial glide and medial tilt is pictured.
Lateral Glide
You can mobilize the patella laterally in much the same way as the medial glide by placing your fingers on the medial border of the patella and gliding it to the outside (laterally).
Inferior Glide
Place your fingers on the top border of the patella. If you are self-mobilizing, you may choose to use the heel of your hand. Gently push the patella toward the foot (inferiorly) until it can not go any further. This mobilization usually feels as though it moves less than the medial or lateral glide.
It can be helpful to place a towel roll under your knee in order to bend the knee slightly. This helps to gain more access to the patella, however it will tighten the structures that restrict patellar motion a bit. I find that a slight bend allows for a better mobilization in this direction.
Superior Glide
The superior glide is very similar to the inferior glide except that you glide the patella toward your head (superiorly). A slight bend in the knee using a towel roll as described with the inferior glide is helpful with this mobilization too.
Patellar Tendon Mobilization
The patellar tendon is soft tissue that connects the tibia bone to the patella. It attaches to the apex of the patella -the lower border - and the tuberosity of the tibia bone - the bony bump you can feel under the patella. Its function is to offer a means of extending the knee through force applied from the quad muscles. The region around the patellar tendon is a common area of scarring.
To find the patella tendon, locate the medial and lateral border of the patella and follow it to downward to the lower portion of the patella. When you can not feel the bone of the patella anymore, feel for a soft, cord-like structure. If you tighten your quad muscles, you will feel the tendon become taught. This is a way to check if you are on the right structure.
Place one finger lateral to the tendon and the other medial. Push the tendon side to side (lateral to medial) to its maximal excursion.
Quad Tendon and Suprapatellar Region
The quad tendon connects the quad muscles to the patella. It lies over the suprapatellar pouch, which is an extension of the knee joint capsule. This is an area where swelling usually appears first.
To mobilize these structures, place your fingers above the patella and move the tissue side-to-side, as if you are massaging the muscle just above the patella. The quad tendon and the suprapatellar pouch are not easy structures to palpate and are not very distinct from one another. With this in mind, do not be discouraged if you do not feel much when you are mobilizing here.








PREVIOUS PART: Principles of arthrofibrosis rehabilitation
NEXT PART: Restoring Quad function
Mr Dirk Kokmeyer

Dirk Kokmeyer PT, DPT, PhD is a physical therapist in Portland, Maine and a board certified sports specialist (SCS) and Certified Orthopedic Manual Therapist (COMT).
He was previously...read more