Some unfortunate knee patients find their progress with rehabilitation frustrated by issues related to adhesions and scarring inside the knee cavity.
This can happen to anyone, but in a particular group of people who seem to form an aggressive type of scar tissue their lives are turned upside down as they struggle to find the right people to help them.
What is the normal range of movement of the knee, and what are the MUA and CPM trying to achieve?
 |
normal flexion |
 |
normal extension |
Dr Noyes has published that the normal ROM is usually minus 5 to 143 degrees in women and usually minus 6 to 140 degrees in men (Ref). [The 'minus' numbers reflect the fact that most people can bend their knee a little bit backwards.]
After surgery, it is almost inevitable that the range of movement will decrease. There may be a reduction in the bending amount (flexion) or in the straightening amount (extension) or both. This happens for a number of reasons:
- The knee may be painful from the surgery
- There may be blood or fluid in the knee, physically preventing its range of movement
- The quads muscle may be inhibited, which frequently occurs after an insult to the knee
- There may be sticky strands or adhesions in various places in and around the knee, preventing the tissues from moving in relation to one another
Why are serial lateral X-rays of the patella relevant to the discussion about arthrofibrosis?
The following two illustrations show how the patella gets passively tugged downwards as the scar tissue develops and contracts in the soft tissues under and around the patella.
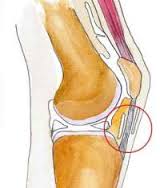 |
Side view of the normal knee showing some of the bursae (lubricating envelopes). Note the normal position of the patella. |
 |
Same view when the envelopes are stuck down with scar tissue, pulling the patella downwards. Note that the patella is now a patella infera (or baja). |
This gradual downward drift can be picked up by the vigilant doctor who is carefully monitoring the problematic patient. The doctor can then pro-actively intervene to break adhesions, keep the knee moving and calm the inflammation down.
References
1. Open Orthop J. 2012;6:199-203. doi: 10.2174/1874325001206010199. Epub 2012 May 16. BMP-2 Dependent Increase of Soft Tissue Density in Arthrofibrotic TKA. Pfitzner T, Röhner E, Krenn V, Perka C, Matziolis G.
